You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
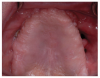
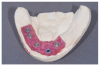
Many patients have been edentulous in both arches for long periods of time with extensive bone loss. Some have very little remaining maxillary bone and a mandibular arch that can receive implants only in the region anterior to the mental foramina (Figure 1 through Figure 3). Removable prosthetic devices, especially those not supported by teeth, offer varying levels of stability in function. Several factors must be considered when designing the occlusal scheme for combinations of completely removable, tooth-supported removable, and implant-supported fixed prosthetics. Air pressure; surface area; peripheral seal residual ridge form and morphology; resistance and retention elements; fulcrum mechanics; and dislodging features require assessment and integration to create a satisfactory prosthetic solution for each patient’s situation.
Atmospheric Pressure
One might ask what air pressure has to do with removable prosthetics. The difference in air pressure from the outside of a denture and the intaglio surface presses the denture against the denture-bearing ridge, similar to the pressure differential that creates lift on the inferior surface of an airplane wing. Atmospheric pressure of 15 pounds per square inch—not suction—applied to the outside surface area is the primary source of retention; there is no vacuum source to create suction (Figure 4).
Peripheral Seal
Peripheral seal is the key requirement for edentulous removable prosthetic retention. Excluding air from the space between the intaglio surface of a removable prosthesis and the denture ridge and the hard and soft tissues maintains the pressure differential. If air gets between the intaglio of a removable prosthesis and residual ridge, the denture will not be retained.
Peripheral seal is achieved with a well-extended impression displacing the border mucosa at the reflection of the denture ridge and mucosa. The post dam in the maxillary arch completes the seal at the vibrating line. Saliva and denture adhesives displace air between the denture and the residual ridge filling this potential space, maintaining the pressure differential.
Surface Area, Residual Ridge Form, and Morphology
McGarry et al provide a classification system for complete edentulism that recognizes different levels of complexity and difficulty when dealing with anatomical conditions present in denture-bearing ridges.1 Many factors, including the extensive vertical and horizontal bone loss, increase the difficulty of providing a stable and retentive removable restoration for a severely resorbed edentulous ridge.
Relative Stability
The concept of relative stability considers which dental arch restoration is more likely to be displaced in function: swallowing, speech, and chewing. Treatment strategies are based on assessment of each situation, applying mechanical principles to provide comfortable and functional restorations balanced to favor and stabilize the prosthetic restoration for the less stable dental arch.
Surface area of an edentulous upper arch is usually greater than the surface area of an edentulous lower arch, enhancing relative stability to the upper arch. Compared with most upper denture ridges, lower denture ridges have much less surface area, remaining topography, and dislodging activity of the tongue and facial muscles contributing to its relative instability. Often the intaglio surface of a conventional lower denture cannot be extended significantly, so air pressure differential to keep it in place is limited.
Locator attachments on implants placed in an edentulous arch dramatically stabilize a removable prosthesis that otherwise would be unstable, similar to the clamp of a meat grinder that attaches to a table or counter, providing antirotation stability (Figure 5). The number and location of implants affect the relative stability of an implant-retained prosthesis. Prosthetics retained by two Locator attachments in an anterior location will flex under occlusal function but will be retained.
Dislodging features include muscle attachments, occlusal contacts during function, tongue volume, and mobility. Resistance and retention features including ridge surface area and residual horizontal and vertical bone morphology resist dislodging features. The stability of all removable prostheses decreases as the volume of bone lost increases.
Chewing Cycle
In order to consider forces applied to removable prosthetics, it is necessary to separate the chewing cycle from the incision of food. Lundeen and Gibbs visualized chewing of different foods as a vertical movement without tooth contact until closure ending in vertical posterior tooth contact.2 The chewing stroke movement occurs lateral to the sagittal plane in a teardrop motion (Figure 6 and Figure 7). A simple way to visualize this pattern is to observe someone chewing food or gum.
Fulcrum Mechanics
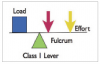
Understanding a Class 1 lever system is basic when designing removable prosthetic occlusal schemes. The Class 1 lever system has a load and lever arm with a fulcrum between them (Figure 8). When an effort (force) is applied near the fulcrum, the load is minimally displaced. When effort is applied farther from the fulcrum, the load is more easily displaced.
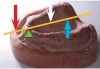
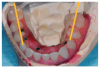
Consider a scenario in which the remaining bone in an edentulous lower arch has resorbed, medially and inferiorly. Visualize each ridge crest as a fulcrum, represented by the green triangles (Figure 9). Starting outside a fulcrum on one ridge crest, extend a line (represented in orange) to the other ridge crest past the ridge crest fulcrum on the other side. A downward force, represented by the white arrow, applied inside the two fulcrums pushes the line against both dental ridges. Force (red arrow) applied lateral to either fulcrum will cause the line to separate from the fulcrum on the opposite side (blue arrow). A similar situation exists in a resorbed upper ridge (Figure 10).
Denture teeth designed to create lingualized occlusal schemes medialize and limit nonvertical vectors of forces when prosthetic teeth contact (Figure 11). These posterior denture teeth are specifically designed to limit contact of upper lingual cusps to the central fossae of the teeth in the lower arch. Phonares II and Physiostar denture teeth (Ivoclar Vivadent, ivoclarvivadent.com)
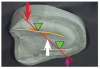
Consider a scenario in a maxillary arch in which bone is lost medially and posteriorly (Figure 12). Beginning anterior to the remaining ridge, extend a line posteriorly to the hard palate, placing a fulcrum on the residual anterior ridge. Force applied anterior to the fulcrum separates the line away from the hard palate. Tooth contact anterior to the anterior ridge fulcrum separates the denture from the palate.
In a situation with extensive maxillary anterior bone loss, anterior tooth contact during chewing results in dislodging the upper denture, especially when the residual ridge has little remaining vertical and horizontal bone. Anterior contact should be avoided, especially in cases with severe resorption of the maxillary bone or against a lower situation that is fixed. Force applied posterior the fulcrum upon closure presses the denture against the hard palate.
Incision of food in dentulous patients is accomplished by gripping food with incisors and hands pulling food forward, away from the teeth, separate from the chewing cycle. Edentulous patients are advised to push food posteriorly when incising against the anterior teeth instead of pulling the food away from the prosthesis to avoid unseating the upper prosthetics.
Cases
Figure 13 shows a situation with a Class III ridge relationship, extensive bone loss in the upper arch opposing a locator-retained lower removable prosthesis. Figure 14 shows that the occlusal contact between the prosthetics is limited to the posterior teeth.
Figure 15 shows a situation with extensive bone loss in both arches. Sinus grafts in the upper arch and implants placed in the grafted sites failed, leaving bilateral oral-antral communication. Revision surgery attaching the buccal mucosa to the residual ridge closed the oral-antral communications, leaving a flat residual ridge with very limited topography (Figure 16). Limited residual bone in the lower ridge determined the asymmetrical location of five implants to provide a screw-retained, implant-supported prosthesis (Figure 17). The residual maxillary posterior ridge crests are medial and posterior the lower arch, opposing a lower implant-retained prosthesis with a Class III relationship to the lower ridge (Figure 18). A lingualized occlusal scheme was designed to limit upper posterior lingual cusp contact to the central fossa of the lower posterior teeth more medial than usual, especially on the lower left side, to stabilize the relatively unstable upper denture (Figure 19). Contact between anterior teeth is avoided during vertical closure while chewing (Figure 20 and Figure 21). Patients are instructed to push food being incised posteriorly against the upper denture to avoid dislodging it, instead of pulling the food forward, as with normal dentitions. Pushing posteriorly seats the denture against the palate (Figure 22).
Summary
When designing occlusal schemes for cases with removable prosthetics, relative stability of the opposing dental ridge arches must be considered. Contact between posterior teeth, especially in severely resorbed dental ridges, is accomplished vertically in a teardrop motion. Occlusal contact upon closure should be limited and lingual to the remaining ridges to seat the least stable prosthesis upon closure.
References
1. McGarry TJ, Nimmo A, Skiba JF, Ahlstrom RH, Smith CR, Koumjain JH. Classification System for Complete Edentulism. J Prosthod. 1999;8:27-39.
2. Lundeen HC, Shryock EF, Gibbs CH. An Evaluation of Mandibular Border Movements: Their Character and Significance. J Prosthet Dent. 1991;40:442-452.
About the Author
Burney M. Croll, DMD
Private Practice
New York, NY
Many patients have been edentulous in both arches for long periods of time with extensive bone loss. Some have very little remaining maxillary bone and a mandibular arch that can receive implants only in the region anterior to the mental foramina (Figure 1 through Figure 3). Removable prosthetic devices, especially those not supported by teeth, offer varying levels of stability in function. Several factors must be considered when designing the occlusal scheme for combinations of completely removable, tooth-supported removable, and implant-supported fixed prosthetics. Air pressure; surface area; peripheral seal residual ridge form and morphology; resistance and retention elements; fulcrum mechanics; and dislodging features require assessment and integration to create a satisfactory prosthetic solution for each patient’s situation.
Atmospheric Pressure
One might ask what air pressure has to do with removable prosthetics. The difference in air pressure from the outside of a denture and the intaglio surface presses the denture against the denture-bearing ridge, similar to the pressure differential that creates lift on the inferior surface of an airplane wing. Atmospheric pressure of 15 pounds per square inch—not suction—applied to the outside surface area is the primary source of retention; there is no vacuum source to create suction (Figure 4).
Peripheral Seal
Peripheral seal is the key requirement for edentulous removable prosthetic retention. Excluding air from the space between the intaglio surface of a removable prosthesis and the denture ridge and the hard and soft tissues maintains the pressure differential. If air gets between the intaglio of a removable prosthesis and residual ridge, the denture will not be retained.
Peripheral seal is achieved with a well-extended impression displacing the border mucosa at the reflection of the denture ridge and mucosa. The post dam in the maxillary arch completes the seal at the vibrating line. Saliva and denture adhesives displace air between the denture and the residual ridge filling this potential space, maintaining the pressure differential.
Surface Area, Residual Ridge Form, and Morphology
McGarry et al provide a classification system for complete edentulism that recognizes different levels of complexity and difficulty when dealing with anatomical conditions present in denture-bearing ridges.1 Many factors, including the extensive vertical and horizontal bone loss, increase the difficulty of providing a stable and retentive removable restoration for a severely resorbed edentulous ridge.
Relative Stability
The concept of relative stability considers which dental arch restoration is more likely to be displaced in function: swallowing, speech, and chewing. Treatment strategies are based on assessment of each situation, applying mechanical principles to provide comfortable and functional restorations balanced to favor and stabilize the prosthetic restoration for the less stable dental arch.
Surface area of an edentulous upper arch is usually greater than the surface area of an edentulous lower arch, enhancing relative stability to the upper arch. Compared with most upper denture ridges, lower denture ridges have much less surface area, remaining topography, and dislodging activity of the tongue and facial muscles contributing to its relative instability. Often the intaglio surface of a conventional lower denture cannot be extended significantly, so air pressure differential to keep it in place is limited.
Locator attachments on implants placed in an edentulous arch dramatically stabilize a removable prosthesis that otherwise would be unstable, similar to the clamp of a meat grinder that attaches to a table or counter, providing antirotation stability (Figure 5). The number and location of implants affect the relative stability of an implant-retained prosthesis. Prosthetics retained by two Locator attachments in an anterior location will flex under occlusal function but will be retained.
Dislodging features include muscle attachments, occlusal contacts during function, tongue volume, and mobility. Resistance and retention features including ridge surface area and residual horizontal and vertical bone morphology resist dislodging features. The stability of all removable prostheses decreases as the volume of bone lost increases.
Chewing Cycle
In order to consider forces applied to removable prosthetics, it is necessary to separate the chewing cycle from the incision of food. Lundeen and Gibbs visualized chewing of different foods as a vertical movement without tooth contact until closure ending in vertical posterior tooth contact.2 The chewing stroke movement occurs lateral to the sagittal plane in a teardrop motion (Figure 6 and Figure 7). A simple way to visualize this pattern is to observe someone chewing food or gum.
Fulcrum Mechanics
Understanding a Class 1 lever system is basic when designing removable prosthetic occlusal schemes. The Class 1 lever system has a load and lever arm with a fulcrum between them (Figure 8). When an effort (force) is applied near the fulcrum, the load is minimally displaced. When effort is applied farther from the fulcrum, the load is more easily displaced.
Consider a scenario in which the remaining bone in an edentulous lower arch has resorbed, medially and inferiorly. Visualize each ridge crest as a fulcrum, represented by the green triangles (Figure 9). Starting outside a fulcrum on one ridge crest, extend a line (represented in orange) to the other ridge crest past the ridge crest fulcrum on the other side. A downward force, represented by the white arrow, applied inside the two fulcrums pushes the line against both dental ridges. Force (red arrow) applied lateral to either fulcrum will cause the line to separate from the fulcrum on the opposite side (blue arrow). A similar situation exists in a resorbed upper ridge (Figure 10).
Denture teeth designed to create lingualized occlusal schemes medialize and limit nonvertical vectors of forces when prosthetic teeth contact (Figure 11). These posterior denture teeth are specifically designed to limit contact of upper lingual cusps to the central fossae of the teeth in the lower arch. Phonares II and Physiostar denture teeth (Ivoclar Vivadent, ivoclarvivadent.com)
Consider a scenario in a maxillary arch in which bone is lost medially and posteriorly (Figure 12). Beginning anterior to the remaining ridge, extend a line posteriorly to the hard palate, placing a fulcrum on the residual anterior ridge. Force applied anterior to the fulcrum separates the line away from the hard palate. Tooth contact anterior to the anterior ridge fulcrum separates the denture from the palate.
In a situation with extensive maxillary anterior bone loss, anterior tooth contact during chewing results in dislodging the upper denture, especially when the residual ridge has little remaining vertical and horizontal bone. Anterior contact should be avoided, especially in cases with severe resorption of the maxillary bone or against a lower situation that is fixed. Force applied posterior the fulcrum upon closure presses the denture against the hard palate.
Incision of food in dentulous patients is accomplished by gripping food with incisors and hands pulling food forward, away from the teeth, separate from the chewing cycle. Edentulous patients are advised to push food posteriorly when incising against the anterior teeth instead of pulling the food away from the prosthesis to avoid unseating the upper prosthetics.
Cases
Figure 13 shows a situation with a Class III ridge relationship, extensive bone loss in the upper arch opposing a locator-retained lower removable prosthesis. Figure 14 shows that the occlusal contact between the prosthetics is limited to the posterior teeth.
Figure 15 shows a situation with extensive bone loss in both arches. Sinus grafts in the upper arch and implants placed in the grafted sites failed, leaving bilateral oral-antral communication. Revision surgery attaching the buccal mucosa to the residual ridge closed the oral-antral communications, leaving a flat residual ridge with very limited topography (Figure 16). Limited residual bone in the lower ridge determined the asymmetrical location of five implants to provide a screw-retained, implant-supported prosthesis (Figure 17). The residual maxillary posterior ridge crests are medial and posterior the lower arch, opposing a lower implant-retained prosthesis with a Class III relationship to the lower ridge (Figure 18). A lingualized occlusal scheme was designed to limit upper posterior lingual cusp contact to the central fossa of the lower posterior teeth more medial than usual, especially on the lower left side, to stabilize the relatively unstable upper denture (Figure 19). Contact between anterior teeth is avoided during vertical closure while chewing (Figure 20 and Figure 21). Patients are instructed to push food being incised posteriorly against the upper denture to avoid dislodging it, instead of pulling the food forward, as with normal dentitions. Pushing posteriorly seats the denture against the palate (Figure 22).
Summary
When designing occlusal schemes for cases with removable prosthetics, relative stability of the opposing dental ridge arches must be considered. Contact between posterior teeth, especially in severely resorbed dental ridges, is accomplished vertically in a teardrop motion. Occlusal contact upon closure should be limited and lingual to the remaining ridges to seat the least stable prosthesis upon closure.
References
1. McGarry TJ, Nimmo A, Skiba JF, Ahlstrom RH, Smith CR, Koumjain JH. Classification System for Complete Edentulism. J Prosthod. 1999;8:27-39.
2. Lundeen HC, Shryock EF, Gibbs CH. An Evaluation of Mandibular Border Movements: Their Character and Significance. J Prosthet Dent. 1991;40:442-452.
About the Author
Burney M. Croll, DMD
Private Practice
New York, NY