You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
Regardless of the clinical situation, patients today demand esthetic restorative outcomes that match their natural dentitions. Traditionally, that expectation has been met by the use of all-ceramic or layered restorations. However, common problems with layered restorations such as fractures and/or chips in the porcelain can contribute to decreased esthetics and function as well as patient discomfort. Such issues can shorten the long-term durability of the restoration. Today, when faced with such challenging cases, the dental team now has the option of using a monolithic zirconia solution as an alternative to layered ceramics.
Case Presentation
A healthy woman in her mid-40s presented for treatment, complaining of a sharp, rough spot on tooth No. 30. Upon examination, the clinician confirmed a mesial lingual cusp fracture on an existing porcelain crown over a milled coping. The dentist could find no evidence of decay, the gingival tissue appeared healthy, and the patient revealed a history of fracturing this crown.
The clinician considered three treatment options: full-cast gold onlay, porcelain-fused-to-metal (PFM) restoration, or an all-ceramic alternative. The final restorative choice needed to be more durable than the existing crown and yet had to be esthetically pleasing. A full-cast gold onlay would not meet the patient’s esthetic demands. The option of a PFM restoration also had limitations due to a history of marginal darkening, which would compromise the esthetics in the long term. In addition, the lower 80-MPa flexural strength of a porcelain bonding to the coping would most likely result in the same negative outcome. The third option, an all-ceramic solution, was discussed with the dental laboratory. The collaborative dental team chose to restore the posterior molar using a Zirlux® FC2 (Zahn Dental, www.zahndental.com) full-contour zirconia monolithic crown, which exhibits more than 1100 MPa. This solution would meet both the durability and esthetic criteria the case required.
The clinician took pre-operative photographs, prepared tooth No. 30 with a shoulder preparation, and photographed the preparation (Figure 1). A vinyl polysiloxane impression was taken of the prepared site and sent to the laboratory along with a bite registration, the photographs, and a prescription for a shade A-1 restoration. The clinician then employed Luxatemp (DMG, www.dmg-america.com) to fabricate a temporary crown. Before dismissing the patient, a follow-up appointment was made for cementation of the new Zirlux FC2 zirconia crown.
The Final Restoration
In the laboratory, a master model was prepared from the supplied clinical impression and then scanned using a Dental Wings 7Series device (Dental Wings, www.dentalwings.com). The laboratory technician used CAD technology to create an anatomically functional crown (Figure 2) and milled the Zirlux full-contour zirconia crown on a Roland DWX 50 milling unit (Roland, www.rolandus.com) using one of the Zirlux preshaded zirconia discs. The fine anatomic detail was achieved, using 0.6-mm and 0.3-mm burs in the 5-axis milling mode. The milled restoration was sintered in the sintering furnace and then using Zirlux stain and glaze material, the restoration was optimized to match the patient’s adjacent natural dentition (Figure 3). The stained and glazed restoration was fired in a Programat P310 porcelain oven (Ivoclar Vivadent). At the certified Zirlux FC2 laboratory, the technician was pleased with the esthetic outcome achieved and delivered the case to the clinician.
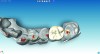
The dentist cemented the completed Zirlux crown using RelyXTM (3M ESPE, www.3mespe.com) and checked the occlusion to confirm the absence of excursive interferences. At the 10-day follow-up appointment, the clinician assessed the occlusion as well as the response of the gingival tissue around the crown. Postoperative photographs demonstrated the natural esthetics of the final restoration. At a 1-year follow-up appointment, the restoration showed no signs of wear or fracture (Figure 4). The clinician and patient were pleased with the result.
Conclusion
The dental team was impressed with the functional durability that Zirlux FC2 offered in the posterior regions because of the material’s monolithic quality. In addition, Zirlux provides highly translucent characteristics, which can be an elusive esthetic quality in a monolithic crown, and offers a cost-effective alternative to traditional layered restorations.
Disclosure
This article was supplied by Zahn Dental.
About the Authors
Sven Jesse, MDT
Sven Jesse is a master dental technician trained in Germany. Mr. Jesse brings almost 30 years of worldwide master dental technician experience to Jesse and Frichtel Dental Labs in Pittsburgh, Pennsylvania. Not only has he successfully taken on the most complex cases but he also has had work published in Contemporary Esthetics, LMT, Dental Lab Products, Dental Implants: The Art and Science, and other publications. Mr. Jesse is a member of the International Congress of Oral Implantologists and American Academy of Cosmetic Dentistry and lectures nationally for Nobel Biocare, Zimmer Dental, and Astra Tech.
Edward Narcisi, DMD
Edward Narcisi, DMD, is an experienced general, restorative, and cosmetic dentist serving the Pittsburgh area. A member of the American Dental Association, Pennsylvania Dental Association, American Academy of Cosmetic Dentistry, and the Academy of Osseointegration, Dr. Narcisi is an active member in dentistry and stays abreast of the latest developments in dental science. In addition to private practice, Dr. Narcisi serves as the clinical codirector of the Multidisciplinary Implant Center at the University of Pittsburgh and codirector of the general practice residency program at the University of Pittsburgh Medical Center Shadyside Dental Center.