You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
A primary issue related to lose of bone and gingival inflammation that is identified as peri-implantitis is related to the design of the prosthetics and trapping oral biofilm. Prosthetic designs to reduce the risk of peri-implantitis should apply prosthetic principles developed for tooth supported prosthetics to reduce the risk of periodontal diseases. Peri-implantitis and Periodontitis are similar bacteriologically, pathologically, and histologically. These designs facilitate effective patient oral hygiene maintenance reducing bacterial plaque accumulation at the interface, the Free Margin of the Gingiva, (FMG) between implants and the intaglio surfaces of implant supported prosthetics. The literature reports that inaccessibility to the prosthetic-implant interface increases the risk of peri-implantitis and the subsequent loss of osseointegration. Direct communication and collaboration are essential between the patient, dentist, dental technologist, and dental hygienist applying established principles to facilitate oral hygiene measures reducing the risk of peri-implantitis. Currently there are limited design recommendations for dentists and dental technologists to design and produce implant supported prosthetics within the limitations of the current production processes. Evaluation of the patient's ability to comply with oral hygiene maintenance should be considered when choosing the best design for each situation. Post insertion instruction by dental hygienists for long term compliance to reduce the risk of peri-implantitis is paramount.
Bacterial Plaque as a primary etiologic factor in periodontitis and peri-implantitis
Peri-implantitis is defined as a bacterial plaque-associated pathological condition related to oral biofilm occurring in tissues around dental implants, characterized by inflammation in the peri-implant mucosa and subsequent progressive loss of surrounding bone1-8(Figure 1 and Figure 2). Food impaction is a contributing but not a primary factor in the disease process.
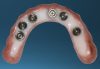
Several factors increasing the risk of peri-implantitis have been reported. Lack of access to the intaglio surface of the implant-supported prosthetics and poor oral hygiene of the implant is reported to increase the risk of peri-implantitis (Figure 3 through Figure 5). Concave intaglio design prevents oral hygiene access (Figure 6). Monje reported that 77.2% of the peri-implantitis cases had inadequate access for cleansability. 9 Serino and Ström found that 74% of the implants had no access to proper plaque control and highlighted the role of prosthesis design.10 Katafuchi suggested that a shallow emergence angle (EA) with a straight or concave transmucosal profile at the interproximal sites should be considered to minimize peri-implantitis risk for bone-level implant.11
Implant supported restorations, like tooth supported restorations, must be designed to function effectively while offering access for oral hygiene maintenance. Studies of natural teeth demonstrate that restoration contours (emergence profile) affect the periodontal health. Perel,Herlands, Youdelis, and Ramfjord reported over-contoured natural tooth supported restorations are a greater periodontal hazard than under-contoured restorations.12-15 Eissmann recommended the interproximal embrasure area in fixed dental prosthesis to be concave to provide access and facilitate oral hygiene maintenance.16 Croll identified normal profiles of natural teeth utilizing photographic analysis revealing straight axial profiles, Emergence Profiles, (EP) present from the base of the gingival sulcus past the FMG into the oral environment.17 Geometric analysis demonstrates that flat EPs for fixed restorations on teeth facilitate convenience and effective oral hygiene procedures approximating the gingival sulcus.18 These concepts hold true for restorations approximating the peri-implant sulcus.
Yi identified influence of prosthetic features that increase and decrease the risk of peri-implantitis through comprehensive analysis.19 There is a positive correlation between the amount of marginal bone loss (MBL), the emergence angle (EA), and convex Eps, and the risk of peri- implantitis (Figure 7). The risk is significantly raised with the increase in the EA (>30 degrees) and the prevalence of peri-implantitis in the convex group. In addition, splinting adjacent implant-supported restorations was identified be a significant risk indicator, particularly position of implants whether, splinted-mesial; middle; or distal) (Figure 8). Yi reported the influence of the EA and the EP on the MBL in the bone-level group for both external and internal connection types, but not the case for the tissue-level group.19 The high prevalence of peri-implantitis in the splinted-middle group may be explained by the limited accessibility for oral hygiene. When adequate cleansability is possible through proper access, the risk of the splinted-middle group to develop peri-implantitis should decrease.
Oral Hygiene Management
Many factors should be considered when designing implant-supported restorations to reduce the risk of peri-implantitis affecting physical removal of bacterial plaque at the FMG. Included are oral hygiene devices, accessibility, prosthetic shapes, and patient ability to comply with oral hygiene procedures. The design should be conveniently hygienic so patients can easily comply with the recommended oral hygiene procedures. Physical removal of bacterial plaque on the intaglio surface at and above the FMG reduces the risk of peri-implantitis in the sub-gingival transmucosal tissue around dental implants. The original fixed prosthetic design presented by Branemark, a "High water design", provided access to all surfaces for oral hygiene management without a patient complaint of food accumulation (Figure 9 and Figure 10). Notably, relief above the gingiva was not patient complaint with this design. Lack of embrasure access to the FMG and intaglio surfaces for oral hygiene management can lead to peri-implantitis (Figure 11 and Figure 12). Stein recommended a convex modified ridgelap pontic design with lingual and palatal access to facilitate plaque removal from the intaglio surface under pontics in fixed prosthetics with dental floss.20 These shapes should be standard for fixed implant-supported restorations whether individual or multi-unit restorations made of ceramo-metal or milled zirconia (Figure 13 through Figure 16).
Commonly available oral hygiene devices include manual and mechanical toothbrushes, irrigation devices, dental floss with threaders and proxi-brushes. To be affective, all devices must have access to reach the prosthetic-implant interface to remove the oral biofilm. Rotary mechanical brushes may not reach the interface as well as straight bristles that can be directed to the interface. In areas difficult to reach, especially in multi-unit posterior restorations, 2 mm relief of the intaglio surface from the soft tissue provides improved access for toothbrush contact for plaque removal (Figure 17 and Figure 18). Water Flossers or Air Flossers without toothbrushing does not adequately remove oral biofilm.21,22 Dental floss with threaders when used properly are effective in disrupting the oral biofilm if the intaglio surface is convex and the patient has the necessary manual dexterity to thread the floss into those areas.
Transmucosal Connection to Implants
In the natural dentition, embrasures provide access to reach the bacterial plaque at the FMG. Flat axial Emergence Profiles have been established to be convenient and effective for patients to reach and remove oral biofilm from natural tooth surfaces.18
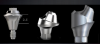
Following the recommendations of Yi, the transmucosal portion of the prosthetic connections should be flat or concave in profile diverging no more that 30 degrees from the long axis of the implants.19 Standard abutment profiles which are flat or convex in profiles are good examples to follow (Figure 19). Following Yi's recommendations individual posterior custom abutments with narrow implants should have flat or concave transmucosal profiles like a standard implant abutment with convex intaglio shapes like pontics that are cleanable with dental floss19 (Figure 20 through Figure 28).
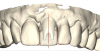
Individual anterior custom abutments should have straight or concave transmucosal profiles extending to the desired gingival line at the FMG (Figure 29 through Figure 35).
Ti-base units, where the microgap is subgingival should follow this design (Figure 36 and Figure 37).
Intaglio Profiles in Edentulous Areas
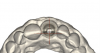
The profiles of the intaglio surfaces facing edentulous areas should be convex like modified ridgelap and ovoid pontics, so these surfaces are accessible and cleanable (Figure 38 through Figure 41).
Patient Factors that May Contraindicate Fixed Implant-supported Prosthetics
At the initial patient examination, several factors in addition to restoration shape should be considered when planning implant-supported restorations. History of periodontal disease, irregular maintenance visits, clinical appearance of the remaining teeth and soft tissue conditions may indicate increased risk of peri-implantitis. Patient dexterity, adaptability, willingness, and capability to carry out intended home care should be considered. Patient's mental conditions including dementia may influence the design of this as well as unrealistic patient expectations. A "High water original Branemark design" or no treatment may be indicated. Especially when implant location makes access, a fixed-removable design may be necessary to reduce risk of peri-implantitis may be indicated (Figures 42 through Figure 45). Considering that oral biofilm accumulation, even at two weeks post prosthetic insertion is documented, periodic removal of screw retained restorations is less effective than daily access to disrupt bacterial plaque accumulation.
Laboratory Production Workflow
Collaboration within the dental team is essential based upon understanding of design principles and oral hygiene management. Prosthodontists, periodontists, oral surgeons and general dentists place dental implants sending digital or analog impressions and working casts to the dental laboratory for prosthetic fabrication. Dental technicians may consult a digital library to design restoration utilizing standard or custom abutments. Often restoration designers have little or no formal technical training or biologic understanding when designing complex restorations and custom abutments. Dental technicians may discuss the design recommendation with the prescribing dentist and provide a PMMA trial shape for try-in requiring modification recommendation and dentist's recommendations. Ultimately, the providing dentist is responsible for supervising the appropriate restoration design. Prosthetics are then delivered for placement following the dentist's approval.
Reducing the risk of Per-implantitis with Long Term Oral Hygiene Management
Long term follow-up care reduces the risk of peri-implantitis requiring shared responsibly between the patient and all members of the dental team. It is becoming common practice for all members of the multi-disciplinary team, dentists, hygienist and dental technicians to interact with the patient during design and placement of implant supported prosthetics. Patients must be made aware that the same disease processes that cause tooth loss may lead to implant failure. Each member of the team must be aware and able to discuss with the patient the importance of design and compliance with oral hygiene management to reduce the risk of peri-implantitis and the possibility of implant loss. The role of the dental hygienist cannot be overstated. Daily physical debridement is key, considering patient dexterity and adaptability. Explaining the prosthetic design shapes and reinforcing patient compliance at recall visits is essential.
References
1. Berglundh T. Armitage G. Araujo MG. Avila-Ortiz G. Blanco J. Camargo PM. Zitzmann N. Peri-implant diseases, and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. Journal of Clinical Periodontology 2018; 45:(Suppl 20), S286-S29
2. Sokransky S et al The microbiota of the gingival sulcus area in Man Total microscopic and viable counts and counts of specific organisms. Arch Oral Bio 1963 8:275-280
3. Ivanovski S., Comparison of peri-implant and periodontal marginal soft tissues in health and disease. Periodontogy 2000 76(1), 116- 130
4. Zitzmann N., Berglundh T., Marinello CP., Linde J., Experimental peri-mucocitis in man. J Clin Periodontal 2001: 28 517-523
5. Buddula A., Bacteria and Dental Implants. J Dent Implants 2013 3(1):58-61
6. Linde J., Berglundh T., et al Experimental Breakdown of peri-implant and periodontal tissues: A study in the beagle dog Clin Oral Implant Res 1992 3(1) 9-16
7. Renvert S., Persson GR., Pril FQ., Peri-implant health, peri-implant mucositis, and peri-implantitis: Case definitions and diagnostic consideration J Clin Periodontol 20: June 2018 182
8. Loe H, et al. Experimental gingivitis in man 1965 J Periodontal 36:177-187
9. Monje A., Pons R., Insua A., Nart J., Wang LH., & Schwarz F., Morphology and the severity of peri-implantitis bone defects. Clinical Implant Dentistry Related Research, 2019; 1-9.
10. Serino G, Strom C Peri-implantitis in partially edentulous patients: association with inadequate plaque control Clin Oral Implants Res 20(2) 2009 169-174
11. Katafuchi M., Weinstein BF., Leroux BG., Chen YW., Daubert D. M. Restoration contour is a risk indicator for peri-implantitis: A cross-sectional radiographic analysis. Journal of Clinical Periodontology, 2018:45, 225-232.
12. Perel, ML. Periodontal considerations of crown contours J Prosthet Dent 1971;28 627-630
13. Herlands R., Lucca J., Morris M., Forms, contours, and extensions of full coverage in occlusal reconstruction. Dental Clinics of North America, 1962:6, 147.
14. Yuodelis R., Weaver J., Sapkos S., Facial and lingual contours of artificial complete crown restorations and their effect on the periodontium. Journal of Prosthetic Dentistry, 1973;29, 61-66.
15. Ramfjord S. Periodontal aspects of restorative dentistry, J Oral Rehab 1974 1:107-26
16. Eissmann HF., Radke RA., Noble WH., Physiologic design criteria for fixed dental restorations. Dental Clinics of North America. 1971;15(3), 543-568.
17. Croll BM., Emergence profiles in natural tooth contour. Part I: Photographic Observations. J Prosthet Dent 1989; 62:4-10
18. Croll, BM., Emergence profiles in natural tooth contour. Part II: Clinical considerations. J Prosthet Dent, 1990 63(4), 374-379.
19. Yuseung Yi., Koo KI-Tae., Schwartz F., Amara HB., Association of prosthetic features and peri-implantitis: A cross- sectional study. J Clin Periodontol, 2020;47:392-40
20. Stein RS, Pontic-residual ridge relationship: A research report J Pros Dent Mar -Apr 1966
21. On Plaque Removal, Sharma NC J Clin Dent 2012 23:17-21
22. Pons R., Nart J., Valles C., Salvi GE., Monje A., Self-administered proximal implant-supported hygiene measures and the association to peri-implant conditions. J Periodontal. 2021; 92:389-399.